
Case Report | DOI: https://doi.org/10.31579/2578-8868/050
1 Resident, Department of neurosurgery, Bangabandu Sheikh Mujib MedicalUniversity, Shahbag, Dhaka, Bangladesh
2 Professor, Department of neurosurgery, Bangabandu Sheikh Mujib MedicalUniversity, Shahbag, Dhaka, Bangladesh
*Corresponding Author: Bipin Chaurasia, Resident, Department of neurosurgery, Bangabandu Sheikh Mujib Medical University, Shahbag, Dhaka, Bangladesh
Citation: Nwoshin Jahan, Nath HD, Mahbub AA, Arifin SA, Baniya P, et al. (2019) Pineoblastoma at Right Frontotemporal Sellar Suprasellar and Parasellar Region: A Rare Case Report. Neurosci Neurol Surg. 4(1); Doi:10.31579/2578-8868/050
Copyright: © 2019 Jahan N, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 28 May 2019 | Accepted: 07 June 2019 | Published: 12 June 2019
Keywords:
Pineoblastoma is a tumor derived from primitive neuroectodermal cells. It is a highly malignant tumor in pediatric age groups. The prognosis of pineoblastoma is very poor than other supratentorial primitive neuroectodermal tumors (PNET). Pineoblstoma arises from pineal parenchyma. We report a case of 2 years boy with history of several episode of convulsion and gradual weakness of left side of body with altered level of consciousness. On MRI (magnetic resonance imaging) it revealed a mixed intensity lesion on right frontotemporal region mainly in the frontal and temporal base. After evaluation we did right frontotemporal craniotomy and debulking of tumor histopathology revealed pineoblastoma which was confirmed by immunohistochemistry.
Primitive neuroectodermal tumors (PNETs) are a group of highly malignant tumors composed of small round cells of neuroectodermal origin. Cranial PNETs are commonly located infratentorially in the cerebellum and are rarely supratentorial. PNET and pineoblastoma both are account for 4.8% & 0.6% of childhood brain tumor [1]. These tumors are common primary central nervous system tumors in children, but they are extremely rare in adults, representing less than 0.5% of all intracranial tumors. Pineoblastomas arise from pineal parenchyma which are a category of supratentoreal PNET. Though pineoblastoma arise from pineal gland we report a case of pineoblastoma which arises from sellar suprasellar area with extension to anterior frontal and temporal base. There are no published case of pineoblastoma which arises from sellar suprasellar area as a primary site. In contrast there are some published series of recurrence of pineal tumor in suprasellar area after removal of tumor from pineal region [2].
Case Report
A two years old boy from remote area of Bangladesh was admitted in the department of neurosurgery, Bangabandhu Sheikh Mujib Medical University with the complaints of one episode of seizure which was tonic clonic in nature, involved all four limbs, persisted for 5 to 6 minutes with no history of tongue biting, frothing, upward rolling of eyeball or no history of involuntary passage of urine and faeces. Following the event, he lost his consciousness for an hour. Then he was transferred to nearby hospital and treated conservatively. After that, he was seizure free for one year without any medication. Then his mother noticed progressive weakness of the left side of his body and baby gradually became lethargic & reluctant to feed with occasional vomiting.
On examination, baby was conscious and irritative, with spontaneous eye opening & following the sound of mother and object. Pupil was reacting to light. Ocular motility was normal. OFC (Occipito Fronatal Circumference) was 52 cm. Other examination wasn’t done.
We did CT (computed tomography) scan (Figure -1b) and MRI of Brain (Figure 1a) with contrast which revealed a mixed density lesion involving the right front temporal region with heterogeneous contrast uptake. MRI of Brain with contrast showed mixed intensity lesion with solid and cystic component involving front temporal region.


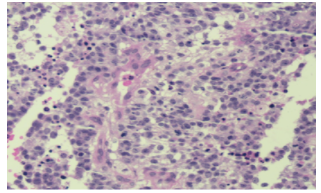

After proper evaluation he underwent right extended front temporal craniotomy and removal of tumor as far as possible. After surgery he symptomatically improved and baby became playful. Histopathology (figure 1c) report reveals pineoblastoma which was confirmed by immunohistochemistry. On 10th postoperative day we discharged the patient with advice to consult with oncologist. Postoperative image showed significant removal of tumor (Figure d).
Discussion
Pineoblastoma is extremely malignant tumor which is locally invasive. It is WHO grade IV tumor which is about <1% of pediatric brain tumors [2,3]. Pineoblastomas are morphologically identical to PNETs in other locations and are similar in their tendency to disseminate through CSF (cerebrospinal fluid) pathway as it is locally invasive so it’s a great challenge to treat such case. The prognosis of pineoblastonma is usually very poor. Several clinical studies have noted that there are important differences in clinical responses to treatment among groups of patients with PNETs arising at different anatomic sites [4] and the reasons for this variations are largely unknown. The location of the PNETs as well as extent of disease at presentation and choice of surgical resection has major importance. Successful treatment requires multimodal approaches with surgery, chemotherapy and radiotherapy. Due to deleterious effect of radiotherapy on developing brain, it is avoided under three years of children [5]. Most of the cases of pineoblastoma present with hydrocephalus. So CSF diversion procedure is another surgical option. VPS (ventriculoperitoneal shunt) & ETV (endoscopic third ventriculoscopy) are common procedure but ETV is most commonly accepted method. Gangemi et al. consider that ETV is not only useful for the treatment of hydrocephalus but also helpful in investigating cells markers, and taking a biopsy [6]. In our case there was mild hydrocephalus. Pineal region was free from tumor .On MRI & CT scan with contrast there was no tumor in the pineal region. So our initial diagnosis was a case of PNET. We didn’t go for any diversion procedure. Rather after optimization we directly went for surgery. Partial decompression of tumor was done due to vessel encasements and severe bleeding. Post-operative period was uneventful & patient improved clinically following surgery. For further management patient was referred to Oncology department.
Survival rate of pineoblastoma is very poor with a median survival of 20 months. Five year survival rate is only 10%. Parikh et al. reported the median overall survival was 34.5 months (range 4.7-183.5) [3]. The prognostic factors of improved survival rates are (1) increased age at presentation (older than 3 years), (2) gross total resection (v/s subtotal or biopsy), (3) lack of disseminated disease and (4) craniospinal radiotherapy more than 40 Gy [7]. The reason of reporting this case is its extreme rarity and very few published cases of pineoblastoma arising from other than pineal region.
Conclusion
Pineoblastoma is very uncommon tumor .Very few cases have been reported in literatures. Those reported cases are mostly from pineal region. Sellar suprasellar pineoblastoma is not reported frequently. As the disease is very malignant surgical decompression, post-operative radiotherapy and chemotherapy increase the median survival rate somewhat. So early diagnosis and treatment is mandatory for the patients’ management and overall survival.
Declaration
Authors’ contributions:
Dr. Haradhon Deb Nath: Conception, diagnosis and design, Radiological diagnosis and Final approval of manuscript
Dr. Nwoshin Jahan, Bipin chaurasia: Manuscript preparation, Technical revision, Maunscript editing and revision
Dr.Nwoshin Jahan, Dr. Abdullah al Mahbub, Dr.Shansul Al Arefin, Dr. Satish Kumar Shah, Dr.Purushottam Baniya: Literature search
Acknowledgement: None
Funding Support and Sponsorship: This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflicts of Interest: There are no conflicts of interest.
Patient Consent: An informed written consent was obtained from the patients parents.
Ethics Approval: There is no ethical issue in this paper.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
